Achilles Tendinopathy (AT) is a common ankle complaint in both the general and athlete populations, with a high prevalence in running and running based sports. Additionally, it is a prevalent condition Melbourne chiropractor Dr. Shannon sees in our sports chiropractic clinic. AT It is a degenerative process tied to overuse and microtrauma, coupled to intrinsic and extrinsic risk factors resulting in pain, swelling and impaired function. Although, there is still limited knowledge in understanding why AT occurs and what process these risk factors play in the development of AT.
Risk Factors
Intrinsic risk factors include:
- Poor vascularity
- Overweight
- Age
- Male
- Lower limb misalignment
- Dysfunctional and weak plantar flexors (calf muscles)
- Reduced flexibility
- Foot/ankle malalignment (flat or high arch)
- Rheumatological and metabolic diseases (diabetes, auto immune disease)
Extrinsic risk factors are mostly tied to training loads, include:
- Training volume
- Distance
- Intensity
- Medication (steroids, fluroquinolones)
Tendinopathy or Tendonitis?
Tendon pain historically has been referred to as tendonitis which reflected the belief that tendon pain was due to inflammation in the tendon; a logical thought process considering tendon swelling is routinely seen in tendon pain. More recently though, through histological examination (looking at tissue cells under a microscope) of tendinopathic tendons (painful tendons) it has become apparent that inflammatory cells are only present in small quantities, with a working theory that these small number of inflammatory cells are present in response to the primary tissue breakdown, not as a direct result of tissue loading. Moreover, there is evidence of cellular apoptosis (cell death) including break down of the cell matrix, infiltration of fatty tissue; an increase in lower quality collagen tissue (type III), proteoglycans (responsible for tendon swelling) and tenocytes, as well as neovascularisation (formation of new blood vessels and nerves) to support the theory that tissue breakdown is responsible for tendon pain and not inflammation.
To add further weight to the argument that inflammation is not a key aspect of tendon pain, research has shown NSAID’s do not enhance early recovery in the treatment in AT, rather it is physical rehabilitation (tendon loading exercises) that aids in the improvement of clinical symptoms. Hence the more appropriate term for local tendon pain associated with tendon-loading activities is ‘tendinopathy’.
How does Tendinopathy occur?
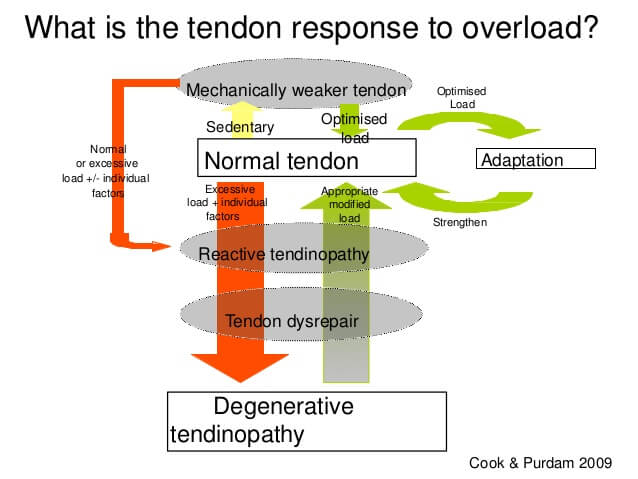
A tendons role is to capture and release energy and one of the current working theories is that this process is disrupted by tendon overload. In a healthy tendon, appropriate load is placed on the tendon, the tissue breaks down as a part of the natural loading process; the tendon then has an appropriate period of rest where it remodels and strengthens; the tendon is then appropriately loaded again and the cycle continues, allowing the tendon to adapt, strengthen and continue its role to capture and release energy.
In a tendinopathic tendon this normal healthy cycle is disrupted either through too much loading, not enough rest or both. Excessive loading of the tendon leads to tissue breakdown, the tissue then doesn’t have enough time to remodel and repair before more load is placed back on the tendon and it continues to breakdown. As that destructive process occurs the tendons ability to capture and release energy is impaired resulting in pain, swelling and dysfunction (tendon pain) leading to a degenerative tendon, this process is called the ‘tendon pathology continuum’. For a more in depth look at the different clinical stages of tendon degradation, read through Melbourne city chiropractor Dr. Shannon’s Chiropractic Australia magazine article on taming Achilles tendinopathy.
Types of Achilles Tendinopathy
AT commonly presents in two ways, either mid portion occurring 2cm or more above the insertion point of the Achilles into the calcaneus (ankle bone) or insertional which occurs within the first 2cm of the tendon from its insertion into the calcanues. Mid portion AT is more prevalent and is seen in approximately 66% of cases.
Achilles Tendinopathy Treatment

There are a myriad of treatment options available for AT these include wait-and-see, night splints, exercise therapy (eccentrics, slow heavy resistance), injection (PRP, cortisone), shockwave therapy, heel lifts, orthotics, acupuncture, tendon scraping under ultrasound, surgery. A recent systematic review and meta analysis looking at a variety of treatment options for mid portion AT was only able to recommend against wait-and-see, as the research for all other treatment options in the study were at risk of bias and/or high heterogeneity, essentially meaning the findings aren’t reliable.
Exercise Therapy For Achilles Tendinopathy
Exercise therapy however, has been more widely researched with a strong focus namely on heavy eccentric and slow heavy resistance programs. Tendon loading programs, more specifically slow heavy resistance rather than eccentrics are thought to help control pain and restore function, via improvements in the tendon’s mechanical strength. How this process actually works is yet to be understood however, a strong tendon means a strong muscle and improved tendon function, strength, motor drive as well as improvements in the overall kinetic chain.
👉 Learn more about how our sports chiropractor Melbourne approaches running injuries.
Injection Interventions for Achilles Tendinopathy
Steroid injections such and NSAID’s are counter productive considering inflammation is not a key driver of the pain and impaired function associated with tendon pain; cortisone can also blunt the tissue healing response. Shockwave therapy in combination with exercise therapy is worth considering particularly in those with insertional AT.
As with any rehabilitation process training loads need to be reviewed and modified appropriately. Avoiding loading the tendon all together is ill-advised as this can lead to tendon degeneration, reduced tendon and muscle strength and stiffness which will flow on impacting the rest of the kinetic chain. Assessment of the lower limb mechanics to establish any imbalances and/or weaknesses is essential and in the case of runners, consideration should be given to foot strike pattern, running speeds, cadence and ground reaction forces via gait analysis.
Achilles Tendinopathy Prognosis
Tendinopathy recovery, including AT takes time with recovery taking anywhere between 3 to 12 months, with some evidence to suggest those with symptoms less than 2 months may experience faster recovery times, whereas those with 3 or more months of symptoms appear to have longer recovery times. Regardless of the duration of your symptoms, being thoroughly assessed and working with a clinician who understands why tendinopathy occurs and what the evidence is currently telling us is best practice in managing tendinopathy will get you back on track faster.
Melbourne city sports chiropractor Dr. Shannon at the Shannon Clinic – Melbourne Chiropractic and Sports Care is well placed to help treat your AT or tendon pain, having worked with elite athletes with in and out of season tendon pain, written articles for his profession and journal papers which have included tendon pain. Click below to book your appointment today.
Read more about the importance of training load monitoring and the services we offer. Additionally, our Melbourne chiropractic clinic is conveniently located in the Melbourne CBD, on Collins Street opposite the Melbourne Town Hall.


