⚽ Injuries in Elite Women’s Football: What Melbourne Athletes Should Know
Sports Chiropractic Insights from Shannon Clinic Melbourne CBD
Following on from the strong interest in the Shannon Clinic – Melbourne Chiropractic and Sports Care’s blog post looking at injuries in elite men’s football during the 2022 FIFA World Cup, and with the 2023 FIFA Women’s World Cup about to kick-off right on our doorstep here in Melbourne, Victoria; Melbourne city chiropractor Dr. Shannon dives into the prevalent injuries seen in elite women’s football to see what injuries might play out at this World Cup.
Women’s football has been growing at a rapid pace, with the number of semi-professional/professional players more than doubling from 1.68 million in 2013 to 3.57 million in 2017. It is now played in over 100 countries, with FIFA working on expanding the number of women participating in football around the world to ~60 million by 2026. But as the women’s game expands, so too should the medical and research support around the women’s game. However, currently there is a scarcity of literature focused on the women’s game, and concerningly 15% of players at the Women’s 2019 World Cup in France played at clubs with no permanent medical staff.
🔍 Key Risk Factors
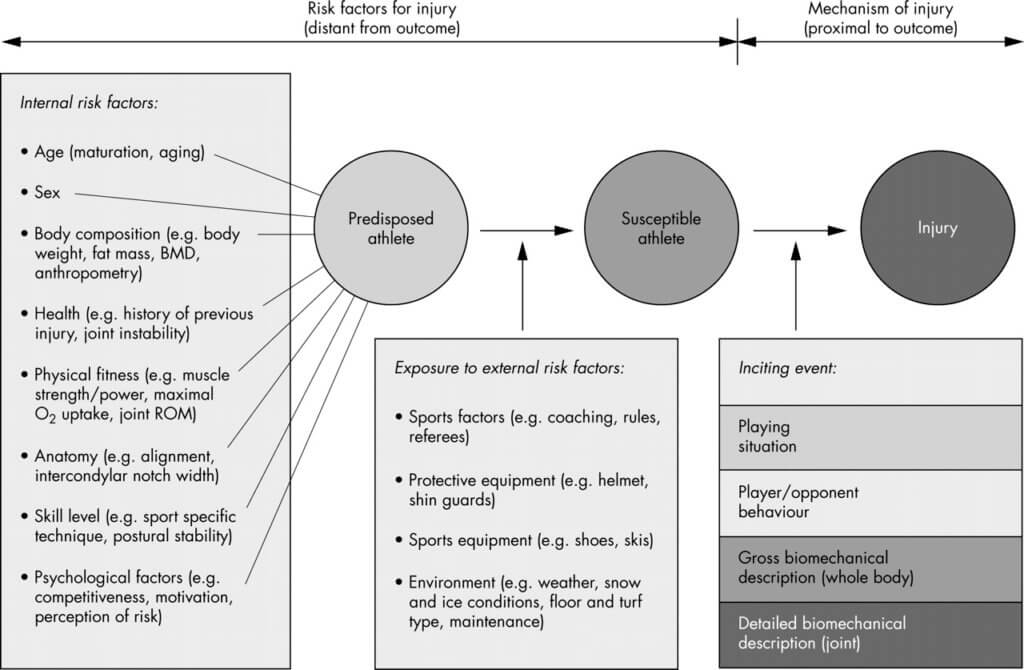
Risk factors associated with an injury are complex and involve both intrinsic factors such as age, sex, BMI, physical fitness/strength and extrinsic factors like equipment, playing surface, weather (figure 1). Specific to elite women’s soccer, intrinsic factors predisposing players to injury include a previous injury, joint hypermobility, age over 25 years old, increased body mass. While specific extrinsic factors include playing position, where defenders and strikers have higher rates of injury than midfielders and goalkeepers.
Risk factors common to both men and women include trait anxiety and negative life events; increased exposure to large and rapid changes in athletic load; being a newly transferred player to a club; positional risks such as low back pain in goalkeepers. Additionally, there are risk factors nominated by elite women players themselves including low muscle strength, poor pitch quality, playing on artificial turf, reduced recovery, hard tackles.
Overall, female players appear to have a higher rate of moderate to severe injury risk than men, as they experience up to 20% more time lost to injury, with evidence suggesting women are at greater risk of ACL ruptures, ankle syndesmosis and quadriceps injuries than men. Additionally, women experience more frequent and severe concussions than their male counterparts.
📊 Injury Trends in Women’s Football
As we have discussed in prior blogs injury incidence or risk rates, that being the risk of sustaining an injury over a specific time frame, can vary in its reporting and football is no exception. Incidence rates can be measured over various time frames including minutes, hours, halves, and matches played, which can make pooling injury data difficult. However, in women’s football per 1,000 hours is a standard exposure time to measure injury risks, and what will be referred to in this blog.
Irish Women’s National League Injury Rates
This paper analyzed injuries in the Irish Women’s National League across two seasons during the 2018 and 2019 seasons.

- Overall injury rates – 7.9/1000
- Injury rates during match play 19.2/1000
- Injury rates during training 2.5/1000
- 50.4% of injuries occurred during match play / 25.1% occurred during training
- 75.6% of injuries had a sudden onset with 45.9% being non-contact in nature
- Injury types – muscle injuries (35%), ligament sprains (30.1%), contusions (9%), meniscus lesions (7.5%), concussion (3.4%), fractures (3.4%)
- Injury site – lower limb injuries accounted for 85% of all injuries
- Injury site by location – ankle (24.4%), knee (21.8%), hamstring (12.4%), achilles/lower leg (7.9%), trunk/spine (6.8%), hip/groin (6.4%)
- Most common injury – lateral ankle sprain (13.9%) and hamstring injuries (12.4%)
- 15% of all injuries were re-injuries with 63% occurring with in 2 months of the initial injury
- ACL injuries accounted for the longest time out with an incidence rate of .2/1000
- 53.8% of injuries occurred in players aged 15-20 years old and 31.6% in players aged 21-25 years old
Systematic Review and Meta-Analysis of Injuries in Elite Women’s Football
This systematic review and meta analysis reviewed studies from 1991 and 2018 that documented injuries in elite women’s football including both play at domestic clubs and at tournaments like the Olympics and World Cup. This blog only references the data from the systematic review, as the meta-analysis had high heterogeneity limiting the quality of the meta-analysis findings (pooling the data together).
Domestic Play
- Overall injury rates during domestic club play 8.4/1000
- Injury rates during domestic club play during match play 30.3-12.6/1000
- Injury rates during domestic club play during training 5.2-1.2/1000
- Injury locations during domestic club play – lower limb accounts for 85% of all injuries. Knee (33%), thigh (21%), ankle (18%)
- Type of injury – ligament sprains (37%), muscle strains (31%), blunt soft tissue trauma (contusions/hematomas) (15%)
- Time lost to injury – 8-28 days (moderate) most common at 34%
Tournament Play – Medical Attention (pitch side)
- Injury locations during tournament play for medical attention (being attended to pitch side) – lower limb accounts for 66% of all injuries. Ankle (24%), head, neck, face (17%), thigh (13%)
- Type of injury – blunt soft tissue trauma (44%), ligament sprain (21%), muscle strain (16%)
- Time loss to injury – 78% of injuries prevented play/training for up to 7 days
Tournament Play – Time Loss
- Overall injury rates during tournament play 11.6/1000 (for time loss)
- Injury locations during tournament play for time loss – lower limb accounts for 89% of all injuries. Knee (22%), lower leg (22%), thigh (17%), ankle (17%)
- Type of injury – blunt soft tissue trauma (42%), ligament strain (21%), muscle strain (16%)
- Time loss to injury – 1-3 days (minimal) most common at 58%
Overall
- Types of injury – ligament injuries (37%), muscle strains (27%), blunt soft tissue trauma (21%)
- Most common diagnosis – ankle ligament sprains (43%), quadriceps muscle strains (16%), knee ligament sprain (12%)
What Does This Injury Data Mean?
At a high level, more injuries occur during match play than training in elite women’s football, which follows a similar trend to men’s football. Furthermore, lower limb injuries consistently account for the largest number of injuries by region, at nearly 90% of all injuries which is again consistent with men’s football. With ligament injuries specifically to the ankle and knee, in addition to hamstring and quadriceps muscle strains making up the bulk of lower limb injuries. This profile is consistent with what we have seen in both elite male and female players.

Additionally, this injury pattern is reinforced by the high rate of sudden onset, non-contact injuries which are consistent with hamstring and quadriceps muscle strains and ligament injuries, especially ACL injuries. ACL injuries is an area warranting further research to understand why female football players have a 2.2 times higher incidence risk of an ACL injury compared to male football players, in addition to a higher reinjury rate, 27% compared to 10% in male football players.
👉 What Melbourne CBD women’s football players need to know about ACL injuries in women’s football
With limited and low quality studies at present, it is unknown why women are at higher risk than men. Current hypothesis include, biological differences such as the menstrual cycle (hormonal changes during the menstrual cycle potentially lead to joint hyperlaxity and an increased risk of a non-contact ACL injury), increased femoral condyle ratio, posterior tibial slope, joint hyperlaxity, larger Q angle. Furthermore, a gendered environmental disparity theory has been raised in the last 2 years which postulates women have different access and experience to sports when compared to men; this include coaches, medical staff, training facilities, high performance programs etc which in turn may result in lower skill levels and conditioning, potentially leading to intrinsic risk factors such as higher BMi, weaker lower limb strength, poor neuromuscular control etc.
Injury Areas of Concern
Two areas of concern that stand out are the higher rates of documented head injuries / concussion 3.4% (Irish League) and 17% (medical attention) in women’s football, compared to men 2% documented. In addition to the high reinjury rates (15%). Where there is a high prevalence of injury to the same injured limb, with 63% occurring within 2 months of the initial injury.
It is likely that head injuries are under-reported in the men’s game, however, knowing female football players experience more frequent and severe head injuries than men, more needs to be done to understand why female players are at a higher risk (technique, neurophysiology, anatomy, neck strength? etc) so more can be done to help mitigate the risks, as well as improve the treatment and prevention of female players.
Additionally, the high rate of re-injuries coupled together with the lack of permanent medical support staff at club level, indicates female players are potentially receiving a lower standard of medical care than their male counterparts, resulting in players returning to play too early, and/or receiving inadequate treatment and rehabilitation.
👉 The Shannon Clinic Melbourne shares their insights on the risks of CTE.
Better Support Needed for Women’s Football
As women’s football rapidly expands and participation rates rise, so must the research literature and quality of medical support for women’s football, this includes encouraging women to take up careers in sports science, research and sports medicine as they are currently under-represented. Moreover, the literature on injuries in elite women’s football is sparse, especially in comparison to men’s football. It’s already known that literature on concussion in women is desperately lacking compared to men, and when coupled with women’s football players suffering more frequent and severe concussion than men, it becomes alarming how neglected our female athletes are.
This is further reinforced by a reported history of gender disparity access to permanent medical support staff in elite women’s teams, plausibily resulting indequate access to treatment, rehabilitation, structured injury prevention programs and appropriate return to play assessments, and therefore comes as no surprise that female players have high reinjury rates, often to the same limb. Let’s get behind our women’s soccer players and female athletes to help raise the support and awareness they deserve.
👉 How soon is too soon to return to play following ACL reconstruction? Analysis from a Melbourne Sports Chiropractor.
📍 Shannon Clinic | Melbourne CBD
Located on Collins Street, Shannon Clinic offers expert chiropractic care for female athletes, footballers, and active professionals. At Shannon Clinic, we treat athletes across all levels—and we’re seeing patterns that demand attention, especially among female footballers. Whether you’re recovering from injury or preventing one—we’re here to help.