Recently The Age / Sydney Morning Herald media outlet published an article titled “For decades, an ACL tear meant surgery. New evidence suggests that may be the wrong move.” The article highlights a recent publication in the British Journal of Sports Medicine which uses a systematic review (literature review) and a meta analysis to examine the various outcomes comparing surgery to rehabilitation following an ACL rupture. In short, the study found rehabilitation with the option for surgery performed similarly to surgery.
Surgery has been the primary treatment intervention for active individuals, especially for athletes; however rehabilitation without surgery has been a long viable option for less active individuals and in those that don’t participate in sports involving pivoting / rapid change in direction like cycling. Cadel Evans is a notable athlete who competed at a professional level without undergoing ACL reconstruction (ACLR).
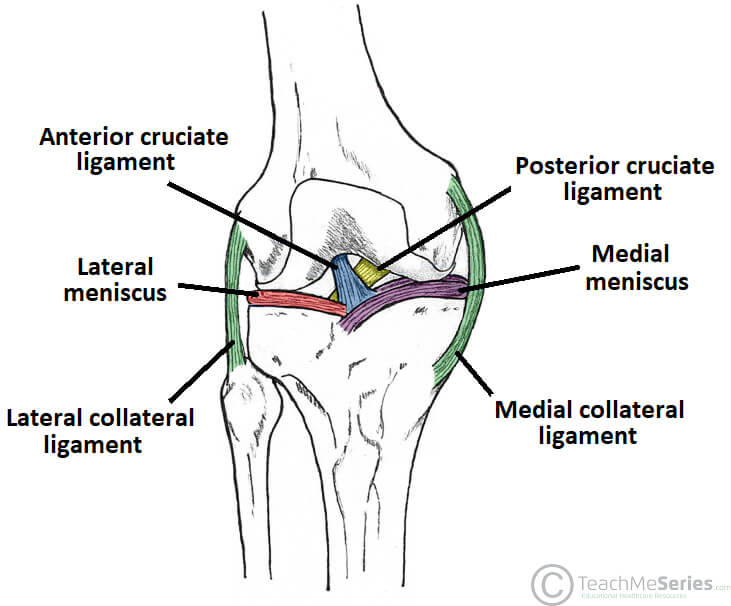
What is the ACL?
The ACL or anterior cruciate ligament is one of two cruciate ligaments in the knee which provides stability to the knee. In the case of the ACL, it’s primary role is to prevent the tibia (shin bone) from sliding forward on the femur (thigh bone) which is called “anterior translation”. Additionally, it plays a role in limiting rotation at the knee, hence it is a key stabilizer of the knee especially when the knee is in a straightened position. When it is ruptured, instability of the knee during pivoting movements becomes apparent in many cases. Hence surgery is often required to reconstruct the ruptured ligament to restore stability to the knee.
Are We Wrong to Be Operating on ACL Injuries?
We need to put some context around the study The Age articles uses to support its narrative. Firstly, The Age article relies on only one study to support their claim, rather than a raft of papers indicating a similar outcome. The author correctly stated the quality of the data is low and hence the recommendations are also low quality. Secondly, on closer inspection the papers inclusion criteria include studies across all age groups, doesn’t exclude for surgery/rehab following re-ruptures, doesn’t stratify by age, sex nor surgical technique, graft type however, does includes randomized controlled trials which is a stronger methodology. Essentially though, this means we are mixing up different groups which can potentially influence the findings. This adds additional weight to suggest the findings of this study are by no means a gold standard even though the methodology was robust.
Further investigation reveals an earlier high quality systematic review which examined randomized control trials comparing surgery to conservative management. Again, the results of this review were low quality due to the high risk of bias. This study on the surface supports the articles claim that there is no difference between patient reported knee function at 2 and 5 years follow up between either group. However, when we dig deeper, we see that the most prevalent complication in the rehabilitation group was instability and by 2 years 39% went for ACLR and by 5 years this had increased to 59%. They also found that the ACLR group had higher return to sport (RTS) rates at 2 years than those in the rehabilitation group.
Return to Sport / Reinjury
The author further highlights the lower rates of RTS and risks of reinjury following surgery as additional arguments for why conservative management could be a viable alternative to surgery. It is important though, to understand what sits behind this data. A systematic review of 1342 recreational athletes found that only 59% returned to pre-injury levels of sport following ACLR, this is slightly higher than the 1/3 stated in the article but provides support for lower RTS rates post-surgery. Another systematic review and meta analysis examining 3744 patients found a similar number (61.8%) of athletes RTS following ACLR. To put context to these low RTS rates we need to consider the psychological impact such a devastating injury has on an individual. That same paper found those who RTS had higher psychological readiness, higher self-efficacy and lower kinesiophobia (movement/joint phobia) compared to those who did not RTS. Furthermore, reinjury risks for ACL ruptures include reduced psychological readiness to RTS. This highlights the importance of the psychological impact of an injury on RTS and may in part help to explain the lower rates of RTS especially in non-elite athletes, rather than associating it with a failure of surgery.
All Groups Are Not Equal
As mentioned earlier the study used to formulate the narrative for The Age article grouped all individuals together and it is known that there are specific subgroups of individuals with different risks and outcomes, males versus females, adolescent versus adults, recreational versus elite athletes etc This isn’t a critcism of the paper, as the data wasn’t available for the authors to undertake a subgroup analysis. However, in youth and adolescents a low quality systematic review and meta analysis comparing surgery to rehabiliation found 20 to 100% in the rehabilitation group experienced instability and only 6-50% in that group RTS. They found early ACLR over delayed ACLR resulted in reduced risks of meniscal tears and irreparable tears. While those in either surgical group had RTS rates of 57-100%. It is also well documented that females, especially soccer players are at greater risk of an ACL injury than males which is postulated to be due to anatomical differences (tibial slope angles).

What About Knee OA?
The author makes a claim that ACLR reduces the risks of osteoarthritis (OA), a claim which they provide no evidence to support. Again, this falls back into all things are not equal and so we cannot group everyone together. It is possible to rupture an ACL and preserve the meniscus. Furthermore, injuries can involve one or both meniscus, as well as the articular cartilage and damage to meniscus and/or cartilage are going to be relevant factors in whether an individual is likely to develop OA. A recent lower quality systematic review and meta analysis examining clinical outcomes and OA 22 years post ACLR found satisfactory outcomes but noted high levels of OA (2.8x compared to the individuals well knee) particularly in those with concomitant meniscal and or cartilage injuries, adding further weight to the argument that cartilage/meniscus injury may play a role in OA development following ACL ruptures.
Furthermore, knee OA following ACLR is a multifactorial process potentially involving factors associated with surgery like an incorrect femoral/tibial alignment but also factors not associated with surgery such as early return to sport, altered lower limb strength and balance. In that follow up study 12.8% had severe OA and only 1.1% went on for a total knee replacement. Melbourne sports chiropractor Dr. Shannon has spent time with orthopaedic knee surgeons in clinical practice and surgery in the US and it is their opinion based on personal experience that the risk of OA increases in patients who delay or do not undergo reconstruction due to the higher likelihood of cartilage injuries.
Where Are We Then?
The narrative for the article is that we have been potentially wrong to operate on those with ACL injuries and perhaps we need to look at alternatives. As has been clearly illustrated in this blog, strong, consistent data is clearly lacking to support a view that we shouldn’t be operating on ACL injuries especially in those active individuals. Injury management options are always weighed up and made based on the circumstances surrounding the individual. Does that mean operating on all individuals with an ACL injury? No. Should the current approach start shifting towards conservative management over surgery? No. More consistent and higher quality data is warranted to make that shift, as has been the case for Achilles tendon ruptures.
You can find out more information about Dr. Shannon and The Shannon Clinic here. If you would like to book an appointment to have your knee assessed, our Melbourne CBD chiropractic practice is centrally located on the corner of Collins Street and Swanston Street, opposite the Melbourne Town Hall in the Manchester Unity building.


