Neck pain and the subsequent disability associated with it is extremely prevalent affecting 55-85% of the global population, and in 2015 it was ranked the 4th leading cause of disability globally. There can be many different aetiologies of neck pain with the more common types including non-specific mechanical neck pain (NSMNP), whiplash associated disorders (WAD), cervical disc radiculopathy, burners/stingers (short lived brachial plexus injuries), cervical cord neuropraxia (short-lived transient disruption of the cervical spinal cord). However, acute neck pain regardless of the cause is often referred to by some clinicians and patients as a “slipped disc” or “pinched nerve”, both erroneous terms and diagnoses. As a sports chiropractor, neck pain is a common presenting complaint and thus the objective of this blog is to differentiate the common causes of neck pain to help you better understand what might be causing your acute neck pain.
Non-Specific Mechanical Neck Pain
NSMNP as the name indicates is neck pain that is mechanical in nature with no clearly defined pain source. The incidence increases with age with the highest prevalence between 45-54 years of age. The onset of NSMNP is often multifactorial, it can be acute or insidious; the pain sharp or dull/achy which maybe localised or referred to another area like the shoulder or upper back (rarely will it refer down the arm); additionally it can be associated with restricted range of motion in the neck. It is the most common type of neck pain we see in our sports chiropractic clinic.
Common clinical presentations we see in our chiropractic clinic include:
- Sporting related such as a choke in Brazilian Jiu Jitsu or being dumped on the ground, motor racing pilots, cyclists
- Lower impact force to the neck such as a slip or fall
- Drying the hair in the morning
- Waking in the morning
- Working longer hours at the desk
Clinical guidelines and systematic reviews recommend conservative treatment interventions involving a multimodal approach utilising patient education, exercise therapy to improve range of motion and neck strength with manipulation/mobilisation, analgesic medication, clinical massage.
Whiplash Associated Disorders
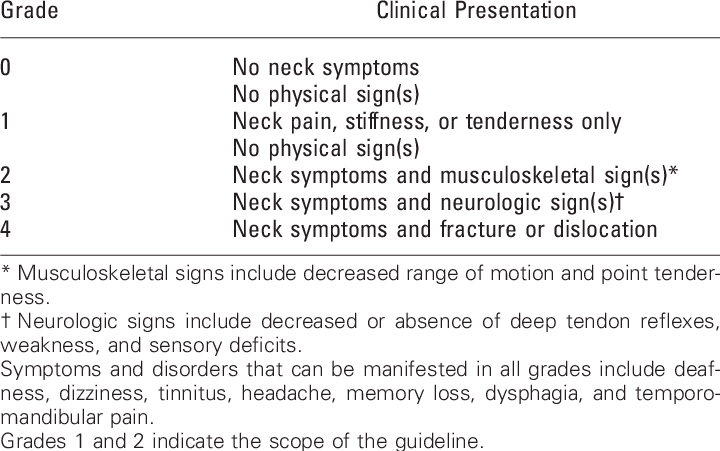
Whiplash associated disorders are cervical acceleration/deceleration injuries which involve rapid displacement of the head and neck in relation to the rest of the body. They most commonly occur in motor vehicle accidents but are seen in collision sports such as rugby, NFL, AFL, ice hockey and may also be a concurrent injury associated with sports concussion (you can read more about whiplash in concussion here). Common symptoms associated with whiplash of which, many also happen to overlap with sports related concussion symptoms include headache, neck, shoulder and back pain, dizziness, numbness, balance/gait disturbance, cognitive difficulties, blurred vision, sleep difficulties, fatigue. WAD’s are graded via a classification system depending on the symptom severity ranging from 0 to IV.
Treamtent for acute (3 or less months) WAD I-III should involve multimodal care including physical therapy (joint mobilisation, soft tissue therapy), analgesics, exercise therapy, psychological strategies (goal setting, relaxation, coping strategies etc). Additionally, for those experiencing dizziness, balance/gait disturbances and/or blurred vision we recommend a more in depth assessment looking at neck proprioception, vestibular-ocular motor function and balance/gait analysis as deficits in these areas usually require more targeted treatment and rehabilitation. You can find out more about how we assess those symptoms here.
Cervical Disc Radiculopathy
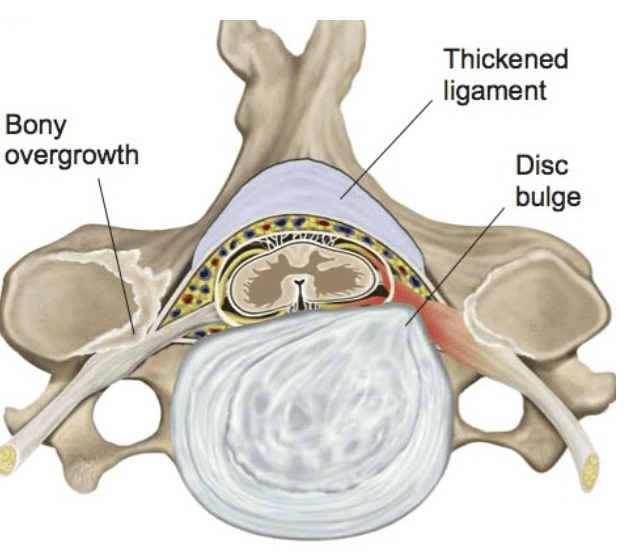
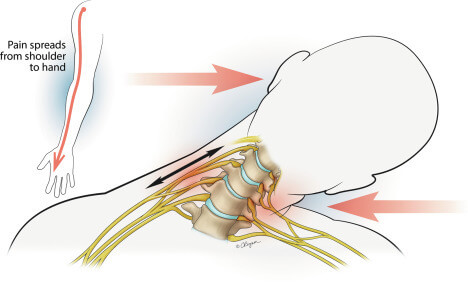
Cervical disc radiculopathy is a common cause of radicular or referred pain with an incidents rate of 5.5/100,000. The aetiology is multifactorial including heavy lifting, occupational such as professional drivers, those who operate vibration equipment, trauma, degenerative disease (arthritis) of the cervical spine. The classic presentation is an onset (sudden or insidious) of severe neck pain with radicular arm pain. Radicular arm pain refers to pain (burning, tingling, shooting pain), sensory (numbness, pins and needles) and motor weakness down one arm and/or forearm/hand. Radicular nerve symptoms are more commonly unilateral (one side) but can be bilateral (both sides) and occur as a result of either a posterolateral (one side) or broader central (both sides) disc protrusion (bulge) or herniation leading to a compression of either one or both exiting nerve roots at the involved level.
Front line intervention for cervical disc radiculopathy is conservative management for 6 to 12 weeks where most cases experience a substantial improvement within 4 to 6 months with full recovery occurring in 24 to 36 months. It is estimated that 26% of patient will require surgery, particularly in cases where neurological symptoms are worsening. Conservative management to aid with pain management includes physical therapy, analgesic medication, steroid injections which may provide relief for 60% of patients while 25% with surgical indications receive short-term relief negating the need for surgery.
Burners/Stingers
Burners and stingers are a transient (short-livid – minutes to hours) injury to the brachial plexus (a large group of nerves positioned around the clavicle) or cervical nerve roots. They are common in contact sports such as rugby, NFL, AFL and are thought to occur because of forceful impact to neck and shoulder area where the neck and shoulder are separated from each other creating a neural traction force. They can also occur as a result of a direct impact over the brachial plexus behind the clavicle or due to extreme neck lateral flexion to one side. This results in short lived neural symptoms including motor weakness or an inability to move the involved limb and/or sensory changes (burning, tingling sensation) down the involved arm/forearm/hand with symptoms usually resolving within a few minutes to hours.
The most common presenting symptoms are sharp pain, reduced neck range of motion and pain down one arm. Weakness and sensation changes in one arm occur in approximately 1/3 of cases which usually resolves within one day. In cases where there are bilateral symptoms or symptoms involving an upper and lower limb then a central cord neuropraxia must be considered, which is an injury to the spinal cord.
Primary management of burners and stingers is through conservative treatment such as physical therapy and exercise therapy with a focus on correcting and strengthening range of motion imbalances in the neck and shoulder.
Concluding Thoughts
There can be a myriad of different reasons why someone is experiencing acute neck pain. This blog has outlined the common causes, how they present and what the best treatment course is. Terms such as “slipped disc” and “pinched nerve” are lazy, non-descriptive and inappropriate. Through a thorough history and examination, it is not a big stretch for a clinician to arrive at the most logical diagnosis and to be able to convey that to their patient in a descriptively accurate and simple manner.
If you are experiencing neck pain be sure to book an appointment with sports chiropractor Dr. Shannon to have your neck assessed. Our Melbourne city chiropractic cliniic is located on Collins Street in the Melbourne CBD and is easily accessible by public transport via tram routes on Collins Street, Swanston Street and via the train at Flinders Street Station, with parking at Federation Square.