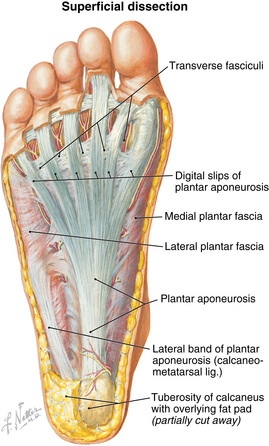
With the 2025 Melbourne Marathon approaching, choosing the best running shoes is crucial for preventing overtraining injuries like shin splints, stress fractures, and plantar fasciitis. Whether you’re tackling the half marathon or full marathon, the right footwear enhances performance and comfort. This guide explores how to select shoes based on your foot type and recommends top models from ASICS, Nike, Brooks, and Hoka to keep you running strong.
Understanding Your Foot Type for Optimal Shoe Selection
A proper foot assessment categorizes runners into one of four types, each requiring specific shoe features to support natural movement and prevent injuries:
Neutral: Balanced foot motion with a slight inward roll (pronation). Most runners (neutral to mild overpronators) fall here.
Mild Overpronator: Mildly flat arch, causing slight inward roll of the ankle/foot.
Severe Overpronator: Flat feet with no arch, leading to excessive inward roll.
Supinator (Underpronator): High arches with minimal or no inward roll.
Identifying your foot type can be performed through a foot and gait analysis at a Melbourne running store or sports clinic— this ensures you choose shoes that provide the right stability, cushioning, or motion control. Most runners are neutral to mild overpronators, making versatile shoes a popular choice.
Top Running Shoes for the Melbourne Marathon by Foot Type
Here’s a curated list of 2025 running shoes from leading brands, tailored to each foot type, to help you conquer the Melbourne Marathon:
Neutral to Mild Overpronator
ASICS Gel-Kayano 31: A premium stability shoe with GEL cushioning and Dynamic DuoMax support, ideal for neutral to mild overpronators. Perfect for long-distance training (lasts ~500–600 km).
Nike React Infinity Run Flyknit 4: Offers plush React foam and a rocker shape for smooth transitions, great for neutral runners seeking comfort.
Brooks Ghost 16: Known for its balanced cushioning and versatility, this shoe suits neutral runners and mild overpronators tackling marathon training.

Severe Overpronator
ASICS Gel-Evolution 7: Designed for flat feet, it provides maximum motion control and arch support to correct excessive pronation.
Hoka Arahi 7: Lightweight with J-Frame technology, this stability shoe prevents overpronation while maintaining a cushioned ride.
Brooks Adrenaline GTS 23: Combines GuideRails technology with responsive cushioning, ideal for severe overpronators needing structure.
Supinator (High Arches)
ASICS Gel-Nimbus 27: A cushioned shoe with PureGEL technology, offering shock absorption for supinators with high arches.
Nike ZoomX Invincible Run Flyknit 3: Features ultra-responsive ZoomX foam, providing ample cushioning for underpronators.
Hoka Clifton 9: Lightweight and highly cushioned, it supports high-arched runners with a neutral platform and meta-rocker design.
Why Shoe Lifespan Matters for Marathon Training
Even if your shoes look new, their internal stability, structure, and shock absorption degrade after a certain distance. For example:
ASICS Gel-Kayano 31: Effective for ~500–600 km.
Nike React Infinity Run: Lasts ~400–500 km.
Brooks Ghost 16: Typically durable for ~500–600 km.
During Melbourne Marathon training, you may log 600–700 km, so replacing shoes mid-season is critical. A smart strategy is to buy two pairs:
Rotate pairs every few runs to extend lifespan and reduce wear.
OR Use a training pair (e.g., ASICS Gel-Kayano) and a race-day pair (e.g., ASICS DS Trainer 19 or Nike Vaporfly 3 for speed).
For amateur runners or those running for fun, the ASICS DS Trainer 19 is a lightweight, responsive race-day option, while the Nike Vaporfly 3 offers a competitive edge with its carbon plate. For runners looking to build foot strength and develop a more traditional barefoot style of running we recommend a progressive transition training program over 3-6 months utilizing minimal shoes such as Altras.
Tips for Choosing Marathon Running Shoes

Visit a Melbourne Running Store or Melbourne Sports Clinic: Get a professional gait analysis to confirm your foot type and try on multiple brands.
Prioritize Comfort: Invest in a couple of pairs of good running socks and ensure a snug fit with enough toe room to prevent blisters during long runs.
Replace Shoes Timely: Track your mileage using apps like Strava or Nike Run Club to know when to replace your shoes.
Test for Race Day: Break in your race-day shoes during training to avoid surprises.
Run Strong in the 2025 Melbourne Marathon
Investing in the right running shoes tailored to your foot type is key to a successful and injury-free Melbourne Marathon. Whether you choose the reliable ASICS Gel-Kayano, cushioned Hoka Clifton, or speedy Nike Vaporfly, prioritize fit and durability.
Managing training loads, building up miles in the legs and hip/leg strength are other key factors in running strong in the Melbourne Marathon. For more assistance or if you are having troubles overcoming a running related injury book an appointment today at our Melbourne CBD clinic for expert advice, and start training with confidence.